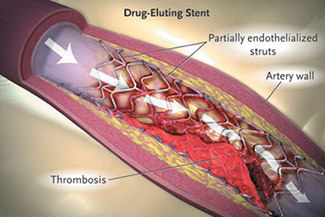
Potential complications
of Coronary Stenting: Late Thrombosis in a Drug-Eluting
Stent
credit: Source:
Curfman, GD. N Engl J Med 2007; published at www.nejm.org
on Feb 12, 2007. Copyright 2007 Massachusetts Medical
Society. All rights reserved |
We may live in an age of astonishing
medical discoveries, but lately it seems that new medicines
and techniques are being discredited faster than they
can be invented. Latest to be touted then doubted is
the drug-eluting stent. If you ever felt that more research
was needed on this technique, your wish has been granted
and then some.
The New England Journal of Medicine
has published five research articles and two commentaries
on the subject over the past month, while another important
review and advisory appeared in the journal Circulation.
Last month the Canadian Medical Association Journal
attacked the problem in some detail. And in December,
the US Food and Drug Administration held a series of
meetings on questions surrounding drug-eluting stents
— meetings that some observers anticipated might
even lead to a suspension of their licence.
That hasn't happened, and it looks
increasingly unlikely. But the FDA remains nervous about
drug-eluting stents, which have been implanted in about
four million Americans. The bugbear that has everyone
so concerned is late thrombosis, a potentially fatal
complication.
A
BAD VIBE
Needless to say, with so many studies coming out at
once, including some that are themselves meta-analyses
of multiple studies, there's something for everyone
in the results. The manufacturers of the two drug-eluting
stents currently on the market claimed to draw comfort
from the research.
But the overall picture that emerged
is rather negative. Not one of the five NEJM
studies found a long-term survival benefit from drug-eluting
stents when compared to bare metal stents. Several found
that drug-eluting stents reduced the need for revascularisation
of the target lesion, but in all cases this benefit
was offset by increased rates of late thrombosis.
There's also concern that even
these latest studies aren't following patients for long
enough. Most of them stretched to three or four years.
But while complications associated with bare metal stents
— namely revascularisation — tend to occur
early, thromboses in drug-eluting stents are often cropping
up later in the study period. The obvious implication
is that with longer follow-up, drug-eluting stents might
prove significantly more dangerous.
MORE
DRUGS PLEASE
The long-term persistence of clotting danger with drug-eluting
stents has given rise to a parallel debate over how
long patients should be given antiplatelet prophylaxis
— usually thienopyridine (clopidogrel or ticlopidine)
in conjunction with aspirin.
But the thienopyridine is often
discontinued as early as three months after stent placement.
There's a growing consensus that this is far too early
even with bare metal stents, and especially with drug-eluting
stents.
Surprisingly, the NEJM research
articles barely address this question. But it is definitely
causing plenty of head-scratching at the FDA. In January,
the journal Circulation carried an advisory from the
American Heart Association recommending 12 months antiplatelet
therapy with all stents. The FDA has now endorsed this
position in a commentary published in the NEJM.
And they're clearly leaving the door open for even longer
extensions.
That means that both drug-eluting
stents on the market, the sirolimus-eluting Cypher stent
and the paclitaxel-eluting Taxus stent, now have inappropriate
labelling, since they recommend three and six months
respectively.
MATH
= TROUBLE
A few back-of-the-envelope calculations can show why
the FDA is so obviously worried by the developing controversy
over drug-eluting stents. Millions of patients already
have them, and the rate of stent thrombosis suggested
by research is at least 1%.
Each stent thrombosis is a grave
event, with two-thirds of cases leading to myocardial
infarction. Death rates from stent thrombosis are estimated
at between 20 and 45% — let's assume 33% for the
sake of argument. That means that even if no more are
implanted, 40,000 Americans are going to have thromboses
in their drug-eluting stents. Twenty-six thousand will
have heart attacks. Thirteen thousand will die.
The really scary news is that these
baseline assumptions come from trials of patients who
met the FDA's approval criteria for drug-eluting stents:
newly diagnosed coronary lesions, less than 30 mm long,
in clinically stable patients without additional serious
medical conditions.
By the FDA's own calculations,
only 40% of patients treated with drug-eluting stents
met these criteria. The rest are getting off-label treatment,
typically for much more serious and complicated conditions.
PENNY
WISE
So where does all of this leave Canada, which approved
these stents a year earlier than the US? Surprisingly,
much better off than might be feared.
We may have dodged the bullet thanks
to the conservatism — what some might prefer to
call the stinginess — of our public health system.
While bare metal stents go for about $800 here, the
drug-eluting stents cost two to four times as much.
In the absence of clear data showing a survival benefit,
Canadian hospitals were loath to shell out the extra
money. So while 80% of stents used in the US today are
drug-eluting, in Canada the proportion is about 30%.
Moreover, percutaneous coronary
intervention is much rarer in Canada. While the US sees
about 750,000 such procedures a year, here there are
only about 35,000, about half as many per capita. So
a Canadian cardiac patient is less than a quarter as
likely as an American to be outfitted with a drug-eluting
stent.
BACK
TO THE FUTURE
A commentary in the Canadian Medical Association
Journal in December noted that in cardiac medicine,
"the interventional community is often accused of making
decisions based on faith more than on fact".
It is indeed hard now to see the
evidence that signposted the route from the treatment
of 30 years ago to that of today. Angioplasty was adopted
without a clear demonstration that it offered a survival
benefit over drugs. Then stents were added without demonstrating
they were better than balloon-only treatment. Then drug-eluting
technology was thrown in without a clear scientific
basis.
Indeed, a December article in NEJM
appeared to bring us full circle. In 2,166 MI patients
with total occlusion of the infarct-related artery,
those randomized to stenting achieved no benefit over
those given simple medical treatment, 1970s-style. The
study questions whether reopening the artery is even
a good idea.
QUESTIONABLE
MOTIVES
The January 16 CMAJ provided what may be the
most enlightening piece of research yet. Researchers
from Holland and from Montreal's McGill University reviewed
the quality, provenance and funding of many of the original
cost-effectiveness analyses of these devices. Of 19
identified studies, 10 supported widespread use and
nine were more cautious.
But only nine studies met criteria
for "high quality", and only one of these recommended
widespread use of drug-eluting stents, compared to nine
of 10 lower quality studies. All seven of the studies
that were sponsored by manufacturers recommended widespread
use, compared to just three of 12 unsponsored ones.
All five studies that came from
the US recommended widespread use. Of the 14 others,
nine were against widespread use, including all four
Canadian ones.
|
Stents: a history
Drug-eluting stents were introduced
to solve the problem of restenosis. Percutaneous
coronary intervention has been around for thirty
years, but in its early days balloon angioplasty
was plagued by very high rates of re-narrowing
of the artery, often within a month. The metal
stent was the obvious solution, getting restenosis
rates down from around 30% to about half that.
But that was still too high.
The drug-eluting stent, introduced here in 2002
and in the US a year later, leaks immunosuppressive
and antiproliferative compounds that prevent tissue
regrowth around it. It has restenosis rates down
to about 4%, a dramatic improvement on the bare
metal stent.
The new devices were approved
following trials with limited follow-up, under
an FDA deal that patients would be further followed
after approval to detect late effects. In the
event, neither the FDA nor the manufacturers'
studies revealed any problems, but soon independent
academic studies began to hint that by three years
after placement, drug-eluting stents had lost
their advantages over bare metal ones and might
even be linked to higher mortality.
|
|







